Introduction
Many women reach the six-week mark after giving birth feeling an urgent pull to move — to reclaim their bodies, their energy, and some version of themselves that predates the exhaustion of new motherhood. The real question is whether the exercise you return to will support recovery or quietly work against it.
Reformer Pilates occupies a genuinely useful place in postpartum recovery. But "postpartum Reformer Pilates" and "regular Reformer Pilates" are not the same thing.
The spring tensions, exercise selection, cueing, and pace all need to be recalibrated for a body that has spent nine months reorganizing itself around a growing human.
Research shows that 60% of women have some degree of abdominal separation at six weeks postpartum, and 31% experience urinary incontinence in the first year after birth. These aren't minor inconveniences: they're signs that the foundation needs rebuilding before intensity can be added back.
This guide covers what pregnancy actually does to the body, why the Reformer is well-suited for recovery, when to start, what early sessions look like, and which movements to prioritize or avoid.
Key Takeaways:
- Medical clearance is a starting point, not a green light for any class
- The Reformer's spring resistance supports foundational work even when core strength is significantly reduced
- Diastasis recti and pelvic floor dysfunction affect most postpartum women and require adapted movement
- Pelvic floor dysfunction isn't always weakness — tightness is equally common and needs different treatment
- Early sessions prioritize breath, connection, and muscle recruitment quality over load or reps
How Pregnancy and Childbirth Change Your Body
Nine months of pregnancy creates changes that don't resolve on their own once the baby arrives. Understanding what has shifted helps explain why a thoughtful return to exercise matters.
The Abdominal Wall and Diastasis Recti
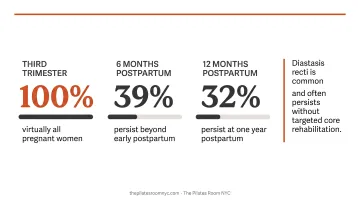
As the uterus expands, the rectus abdominis muscles separate along the linea alba — the connective tissue running down the midline of the abdomen. This separation, called diastasis recti abdominis (DRA), is nearly universal in the third trimester. Studies show prevalence of 66% in the third trimester, declining to around 45% at six months postpartum and 32% at twelve months — meaning roughly one in three women still has clinically significant separation a year after birth.
The problem isn't just cosmetic. A compromised linea alba reduces the ability of the abdominal wall to generate and transfer force efficiently, affecting everything from how you lift your baby to how you stabilize your spine during exercise.
The Pelvic Floor
The pelvic floor is a group of muscles forming the base of the pelvis, supporting the bladder, uterus, and bowel. Both vaginal and cesarean births affect it significantly:
- Vaginal delivery involves direct stretching and potential tearing of pelvic floor muscles and connective tissue
- C-section disrupts the abdominal wall surgically, altering how the deep core and pelvic floor coordinate — even without a vaginal delivery
- Severe perineal tearing (third or fourth degree) occurs in approximately 6% of first-time mothers, requiring additional recovery time before any load is introduced
Postural and Hormonal Shifts
Pregnancy reshapes posture in ways that persist for months. Common patterns include:
- Rounded shoulders from feeding and holding a newborn
- Stiffened ribcage mobility
- Changes to the lumbar curve
Relaxin, the hormone that loosens ligaments during pregnancy, drops rapidly in the first week or two after birth, though levels may stay elevated longer in women who are breastfeeding.
Neurologically, many new mothers experience reduced proprioception (body-position awareness) and altered breathing patterns that developed in the final trimester as the diaphragm was compressed upward. Both factors affect how the body recruits muscles during exercise, which is why resuming your pre-pregnancy routine without modification rarely works.
Why Reformer Pilates Is Especially Beneficial Postpartum
The Reformer isn't just a useful exercise machine for postpartum recovery — its particular design addresses several of the key challenges a postpartum body faces.
Spring Resistance Meets the Body Where It Is
Unlike free weights or bodyweight exercises, the Reformer's spring system can assist or resist movement depending on how it's configured. For a postpartum woman whose deep abdominals and pelvic floor are not yet functioning reliably, this matters enormously.
A footwork series on lighter springs lets the legs rebuild strength without demanding that a depleted core stabilize against significant load. Arm work in the straps can be done in supported supine positions. The Reformer meets the body at its current capacity rather than demanding performance it isn't ready to give.
Classical Pilates Principles Address Postpartum Priorities Directly
The foundational principles of Classical Pilates — breath, centering, control, precision — are not incidental to postpartum recovery. They're central to it.
- Breath directly drives the function of the deep core and pelvic floor. Learning to exhale on exertion and coordinate the diaphragm with the transverse abdominis is one of the most important early steps in postpartum rehabilitation.
- Centering means working from the deep core outward — precisely the approach needed to address diastasis recti and pelvic floor dysfunction without aggravating them.
- Precision over load: early postpartum work is about the quality of muscle recruitment, not how heavy the spring or how many reps.
Physical and Mental Benefits
For the body, adapted Reformer Pilates helps with:
- Rebuilding deep abdominal and pelvic floor function
- Reducing low back pain (one of the most common postpartum complaints)
- Improving ribcage mobility and posture
- Restoring hip and glute strength that often diminishes during pregnancy
For the mind, the connection matters too. A 2024 systematic review found that low-intensity group Pilates one to two times per week improved depression, anxiety, and fatigue in postpartum women. That benefit doesn't happen by accident. Pilates demands sustained internal attention — noticing breath, recruitment, and alignment in real time — which is exactly the kind of focused practice postpartum recovery calls for.
At The Pilates Room NYC, the no-music, no-social-media environment is a deliberate choice that supports this attentiveness — giving postpartum clients the space to move with full presence rather than distraction.
When Can You Start Reformer Pilates After Giving Birth
General Guidelines
The standard guidance most healthcare providers follow:
- Vaginal birth: Medical clearance typically occurs around six weeks postpartum. ACOG notes that after an uncomplicated vaginal delivery, light activity can resume when the mother feels ready — but structured Reformer sessions are a different category from gentle walking.
- C-section: Plan for a minimum of twelve weeks before beginning Reformer work. The surgical incision passes through multiple layers of abdominal tissue, and some women need considerably more time than that.
- Complications (OASI, significant tearing, pelvic girdle pain): These extend both the waiting period and the modifications required once you return.
Medical clearance opens the door — it doesn't determine how far you walk through it. A woman cleared at six weeks is ready to begin a careful reintroduction — not to rejoin a regular group class at normal intensity.
That timeline gives you something useful: a window to prepare.
Before You're Cleared
The weeks before formal clearance aren't empty waiting time. Foundational work can begin immediately:
- Diaphragmatic breathing exercises to restore coordination between the breath, deep core, and pelvic floor
- Gentle pelvic floor awareness (both contraction and conscious release)
- Supported mobility work for the hips and thoracic spine
Done consistently, this groundwork rebuilds the neuromuscular connections that postpartum Reformer work depends on — making your first sessions more productive and your body better prepared for the load.
What Postpartum Reformer Sessions Look Like
The Initial Assessment
Every postpartum body is different — which is why a thorough intake comes before any movement. A qualified instructor needs to understand:
- Type of birth and weeks postpartum
- Any complications (C-section scar, perineal tearing, diastasis recti diagnosis, pelvic girdle pain)
- Current symptoms: leaking, pelvic heaviness, back pain, pain with movement
- Breastfeeding status (affects joint laxity considerations)
- Sleep and energy levels — relevant because a severely sleep-deprived body responds differently to load
Alison Johnson, owner and lead instructor at The Pilates Room NYC, brings both professional depth and personal experience to this work. Having recovered from two C-sections herself and guided many women through prenatal and postnatal movement over 26 years of teaching, she works with each client based on where they actually are.
Early Session Focus
The first sessions are about reconnection, not challenge. A typical early session might include:
- Breathwork and pelvic floor coordination — learning to engage and release, not just contract
- Footwork series in supine (parallel and turned-out positions, bent knee to more extended) — rebuilds lower body strength without loading the deep core
- Supine arm work in the straps (chest expansion, arm circles) — restores shoulder mobility and upper body engagement in supported positions
- Bridging variations — gentle posterior chain activation
- Supported ribcage rotation and extension — addressing the thoracic restriction that develops in pregnancy
Horizontal and semi-reclined positions dominate early sessions, reducing gravitational load on the pelvic organs during the period when the pelvic floor is still healing.
Progression Over Time
Once the foundation is in place, the work builds in a deliberate sequence. As strength, coordination, and body awareness return, sessions evolve:
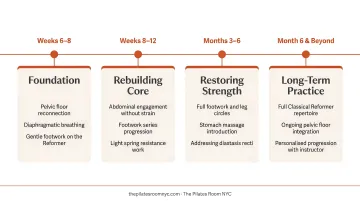
- Weeks 6-12: Foundational breath, pelvic floor, footwork, supine arm and leg work
- Weeks 12-20: Introduction of more varied positions, seated work, gentle rotation
- Beyond 20 weeks: Standing work when pelvic stability is established, single-leg sequences, more demanding abdominal work
- Long-term: Return to the full pre-pregnancy repertoire when the foundation is solid
How quickly a client moves through these stages depends on her birth experience, current symptoms, and how her body is responding — which is exactly why an experienced instructor matters at every step.
Movements to Prioritize and Ones to Avoid
Exercises That Support Postpartum Recovery
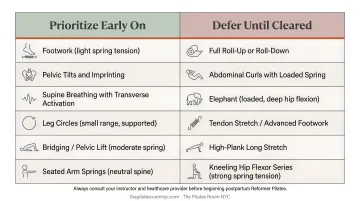
These Reformer movements are appropriate for most women in early postpartum work:
- Footwork series — parallel and turned-out positions, progressing from bent knee to more extended range as strength builds
- Supine arm work in straps — chest expansion, arm circles in supported lying positions
- Frog and leg circles in straps — at low spring tension, focusing on hip mobility without demanding core stabilization
- Bridging variations — posterior chain work that avoids high intra-abdominal pressure
- Supported side-lying leg series — gentle hip strengthening once the client is comfortable on their side
- Seated rowing variations — once the core has enough stability to support upright positions
The goal of these exercises is re-establishing proper muscle recruitment patterns — specifically, learning to engage the deep abdominals and pelvic floor before and during movement. Quality of connection matters far more than load or repetition count.
Exercises to Defer Initially
Some movements place demands on a healing postpartum body that exceed what it can safely handle early on — understanding why helps clarify when to reintroduce them:
- Full planks and push-ups — require significant deep core stability that is typically absent in early recovery
- The Hundred in traditional form (head lifted, legs extended) — generates high intra-abdominal pressure that can worsen diastasis recti and stress the pelvic floor
- Sit-ups and roll-ups — a 2015 study on Reformer intra-abdominal pressure found roll-up movements generate higher cumulative IAP than sit-to-stand; these should wait until the core is rebuilt
- Asymmetrical single-leg loading (scooter, side-lying foot-in-strap work) — until pelvic stability is confirmed, these can aggravate pelvic girdle pain
- Balance-intensive standing carriage work — until proprioception and lower body strength have genuinely returned
Heavy loading, breath-holding, and aggressive bracing all spike intra-abdominal pressure — the common thread in each movement above. As deep core and pelvic floor strength return, most of these exercises can be reintroduced gradually and with attention to symptom response.
Special Considerations: C-Section, Diastasis Recti, and Pelvic Floor
C-Section Recovery
C-section recovery requires a longer return timeline and a more specific approach than vaginal birth recovery. The surgical incision passes through multiple tissue layers — skin, fascia, muscle — and scar tissue formation affects how the deep abdominals recruit during movement.
Before beginning Reformer work after a C-section, scar tissue mobilization with a pelvic health physiotherapist (typically starting around six to eight weeks post-surgery) can significantly improve how the abdominal wall responds to training. An instructor with C-section experience will cue abdominal engagement differently in early sessions, avoiding pressure directly over the scar and building load very gradually.
Diastasis Recti
Most women have some degree of abdominal separation after a full-term pregnancy. Adapted Reformer Pilates addresses this through:
- Prioritizing transverse abdominis activation, which draws the abdominal wall inward rather than pushing outward
- Avoiding rectus-dominant movements like crunches and sit-ups, which can widen separation in the early postpartum period
A pelvic health professional can measure diastasis recti accurately — ultrasound is more reliable than the finger-width self-test. That said, a basic self-check (pressing fingers along the linea alba above, at, and below the navel during a small head-lift) gives a general sense of what's present. Professional assessment before starting postpartum Pilates gives you and your instructor the clearest picture to work from.
Pelvic Floor: Not Just Weakness
This is widely misunderstood. Postpartum pelvic floor dysfunction is not always about muscles being too weak. Some women have a hypertonic (too-tight) pelvic floor — one that needs to learn to release as much as it needs to contract.
Symptoms like pelvic heaviness, urgency, or pain with movement can indicate tightness rather than weakness. Doing Kegel exercises when the pelvic floor is already too tight can worsen symptoms rather than resolve them.
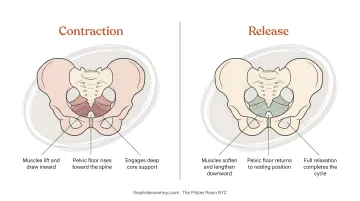
A well-designed postpartum Pilates session trains the pelvic floor through its full range — engaging during exertion and consciously releasing during rest phases of each exercise. The International Continence Society defines pelvic floor muscle training as exercise to improve strength, endurance, power, relaxation, or a combination — not contraction alone.
Frequently Asked Questions
Is Reformer Pilates good for postpartum?
Yes. The Reformer's spring-assisted resistance allows foundational exercises to be performed with proper mechanics even when core strength is significantly reduced after birth. Classical Pilates principles — breath, centering, controlled movement — directly rebuild the deep core and pelvic floor function that pregnancy and birth affect most.
When can I go back to Reformer Pilates after giving birth?
General guidance is six weeks postpartum for uncomplicated vaginal birth and twelve weeks minimum for C-section, always after explicit medical clearance. That clearance is not a green light to resume your pre-pregnancy routine — early sessions should be introductory and tailored to your current recovery status.
Can Pilates help a weak bladder after childbirth?
Yes — Pilates rebuilds pelvic floor strength and coordination, which directly addresses postpartum urinary incontinence. Whether the issue stems from weakness or tightness matters, though, since the approach differs. A pelvic health physiotherapy assessment alongside postnatal Pilates tends to produce the best outcomes.
Can I do Reformer Pilates after a C-section?
Yes, but with a longer wait (typically twelve weeks minimum) and specific modifications around scar tissue, abdominal recruitment, and load progression. Working with an instructor experienced in C-section recovery — who understands how scar tissue affects deep core function — makes a meaningful difference to both safety and outcomes.
Can Reformer Pilates help with diastasis recti postpartum?
Properly adapted Reformer Pilates is one of the most effective approaches for diastasis recti. The focus on transverse abdominis engagement — rather than superficial crunch-based work — helps draw the abdominal wall together, and the Reformer allows that to be trained progressively across a range of movements and positions.