Introduction
Knee pain affects approximately 25% of adults, and its prevalence has increased nearly 65% over the past two decades — a trend that shows no signs of reversing. Yet most people respond to knee pain in one of two ways: they rest completely until the pain fades, or they return to exercise too aggressively and make things worse.
There's a more effective path between those two extremes.
Pilates-based knee rehabilitation is a structured, low-impact approach that addresses not just the knee joint itself, but the surrounding muscles and broader kinetic chain (hips, core, and feet) that all influence how load travels through the knee during daily movement.
Clinical research consistently supports Pilates as one of the most effective low-impact methods for knee recovery, and it's accessible at nearly every stage of injury or condition.
This guide covers how Pilates works as a rehabilitation tool, how to move through it phase by phase, which exercises help most, and when professional guidance matters.
Key Takeaways
- Pilates rebuilds the quadriceps, hamstrings, glutes, and hip stabilizers — the muscles that protect the knee under load
- A phased approach is non-negotiable; skipping early work is the most common reason knee pain returns
- The knee doesn't work in isolation — hip, foot, and core dysfunction all feed stress directly into the joint
- Classical Pilates equipment lets you control and gradually increase load, keeping it practical at every rehab stage
- A proper diagnosis before starting is essential — your program must match the specific cause of your pain
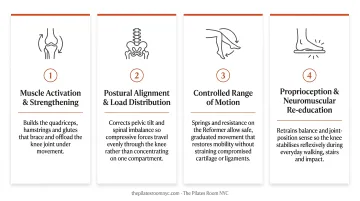
Why Pilates Works for Knee Rehabilitation
The knee is a hinge joint. It bends and straightens. That's its primary job. But how well it does that job depends almost entirely on what's happening above and below it. Tight hip flexors, weak glutes, collapsed arches, and poor core control all create compressive and shear forces at the knee that accumulate over time, contributing to pain and structural wear.
This is why isolated knee strengthening so often falls short. Targeting the quadriceps alone doesn't address the hip rotation deficits or valgus collapse patterns that drove the problem in the first place.
The Clinical Case for Pilates
A 2022 systematic review published in Musculoskeletal Care evaluated seven studies involving 397 participants (mean age 50+, 73% female) and found mat-based Pilates was significantly effective (p ≤ 0.05) for reducing pain and improving physical function and quality of life in people with chronic musculoskeletal conditions including knee osteoarthritis.
A separate RCT of adolescents with patellofemoral pain syndrome found that Pilates-based core strengthening combined with conventional physical therapy significantly improved pain, hip abductor strength, knee extensor strength, and quality of life compared to standard PT alone.
What Pilates Actually Fixes
Several specific mechanisms make Pilates well-suited to knee rehab:
- VMO re-engagement: The vastus medialis oblique commonly shuts down after injury — a phenomenon called arthrogenic muscle inhibition that impairs patellar tracking and destabilizes the joint. Controlled knee extension exercises directly retrain it.
- Patellar tracking correction: When the VMO and hip external rotators are weak, the kneecap pulls laterally under load. Pilates alignment cues and progressive loading address this directly.
- Hip and glute activation: Weak hip abductors and external rotators are associated with increased knee valgus, the inward knee collapse that places the highest stress on the joint during movement.
- Whole-body integration: Pilates uses breath, alignment, and coordinated movement to rebuild balanced musculature without excessive shear force on healing tissue.
Pilates is also adaptable across conditions: osteoarthritis, patellofemoral pain syndrome, and post-surgical recovery all respond well because exercises can be adjusted in range of motion, load, and complexity based on where someone is right now.
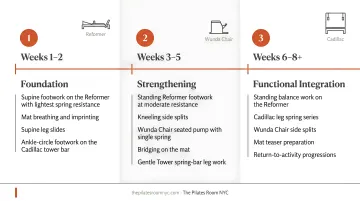
How Pilates Knee Rehabilitation Works: A Phase-by-Phase Guide
Every effective knee rehab program moves through the same progression: reduce pain and restore basic movement, rebuild strength and alignment, then add functional load. Rushing that sequence is the most common rehab error — and it reliably produces setbacks.
Phase 1: Early Rehabilitation (Weeks 1–3)
Goals: Reduce pain and swelling, restore basic range of motion, gently reintroduce the knee to movement.
All exercises at this stage are non-weight-bearing or minimally loaded. The focus is circulation, tissue healing, and re-engaging the nervous system's connection to the muscles around the joint — not strength.
Key Phase 1 exercises:
- Heel slides (supine)
- Clamshells (sidelying)
- Gentle knee bends in supine
- Supine footwork with minimal load
Before progressing: You should be able to move through your available pain-free range without significant swelling or increased discomfort the following day.
Phase 2: Rebuilding Strength and Alignment (Weeks 4–8)
Goals: Active quad and glute strengthening, hip stabilization, and establishing correct alignment under light load.
Key Phase 2 exercises:
- VMO activation (isometric and dynamic)
- Bridging variations
- Straight leg raises
- Seated footwork on the Reformer with light spring resistance
Alignment cues become critical at this stage: the knee must track in line with the second and third toes during any loaded movement. Hip work is equally important. Overactive hip flexors and underactive glutes are a primary driver of poor knee mechanics — lateral hip work using leg springs on the Tower, or sidelying mat exercises, restores balance across the hip and directly reduces stress at the knee.
Phase 3: Progressive Loading and Functional Movement (Weeks 8+)
Goals: Weight-bearing exercises with full knee control, building toward functional strength.
Phase 3 introduces:
- Assisted squats (standing, with support)
- Scooter on the Reformer
- Standing leg pump
- Forward lunges on the Reformer or Chair
Spring-assisted movements are well-suited to this phase. Load can be increased incrementally as strength and confidence improve — a meaningful advantage over bodyweight-only training, where the jump from no load to full bodyweight can be too abrupt.
One critical principle in Phase 3: rotation must come from the hip, not the knee. The knee's job is flexion and extension. Any twisting forces during standing exercises should originate at the hip joint, not be absorbed by the knee's ligamentous structures. Knowing when you're ready to progress through each phase — and when to slow down — is where working with an experienced instructor makes a real difference.
The Best Pilates Exercises for Knee Rehabilitation
Heel Slides (Phase 1)
Setup: Lying on your back, gently slide one heel toward the body along the mat, bending the knee as far as comfortable, then slide it back out.
Why it works: This reintroduces movement at the joint without any loading. It reduces stiffness, stimulates circulation in the surrounding tissue, and begins re-engaging the hamstrings — without asking anything demanding of an inflamed or post-surgical knee.
Shoulder Bridge (Phase 1–2)
Setup: Lying on your back, feet flat and parallel, hip-width apart. Press through the heels and lift the pelvis, engaging glutes and hamstrings. Lower with control.
If you feel pressure or pain at the front of the knee, move your feet slightly further from the body. This exercise has very few contraindications and can be modified for nearly any knee condition.
Clamshells (Phase 1–2)
Setup: Lying on your side, knees gently bent and stacked. Keeping the pelvis still, rotate the top knee open toward the ceiling, then lower.
This targets the hip external rotators — muscles that, when underactive, allow the knee to collapse inward during weight-bearing. Strengthening them here creates the hip stability the knee depends on.
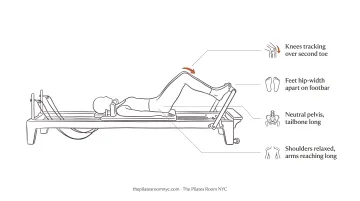
Footwork on the Reformer (Phase 2–3)
Setup: Lying supine on the Reformer, feet on the footbar. Perform controlled knee bends and extensions against spring resistance.
This is a cornerstone exercise in Pilates knee rehab. The Reformer allows precise cueing of VMO activation, controlled range of motion, and progressive loading without impact — all adjustable in real time.
At a studio like The Pilates Room NYC, where Reformers include both wooden and original Gratz metal models, an instructor can fine-tune spring resistance and provide alignment cues that are difficult to replicate on a mat alone. That real-time feedback, particularly for patellar tracking, matters during this phase.
Assisted Squat (Phase 3)
Setup: Standing with feet shoulder-width apart, holding a support (bar, wall, or Reformer frame). Lower into a squat by bending the knees and hips, keeping the knees tracking over the second and third toes. Press through the heels to rise.
This builds functional confidence in the patterns used for sit-to-stand, stair climbing, and daily loading. The alignment principle — knee over toe, not caving inward — must be consistent throughout.
What Affects Your Progress — and Mistakes to Avoid
Several factors shape how quickly you progress through Pilates knee rehab:
- The type and severity of the initial injury
- How long the problem has been present
- Compensatory movement patterns the body has developed in response to pain
- Consistency of practice
Most people see meaningful improvement within 4–8 weeks of consistent work — though this is a measurement window, not a recovery guarantee.
The Most Common Mistakes
1. Knee valgus (collapsing inward) Valgus collapse during squats, lunges, or even walking places enormous stress on the medial structures of the knee. It typically stems from weak hip abductors and external rotators, which is precisely why hip work belongs in every phase of a knee program. Of all the patterns to watch for, this one causes the most damage.
2. Skipping Phase 1 When pain is mild, Phase 1 can feel unnecessary. It isn't. The neural inhibition that shuts down the VMO after injury doesn't resolve just because pain has faded. Skipping early activation work means building later-phase strength on a still-dysfunctional foundation.
3. Pushing through sharp or worsening pain Mild discomfort during movement is expected. Sharp pain during an exercise, or significantly increased soreness the following day, is a signal to stop, modify, or consult a professional.
4. Neglecting recovery basics outside sessions What happens between sessions matters too. Three factors often overlooked:
- Sleep: Quality rest is when tissue repair actually occurs
- Protein intake: Adequate protein supports muscle rebuilding after loading
- Footwear: Very flat, unsupportive, or backless shoes affect knee loading mechanics throughout the day
When Pilates Alone May Not Be Enough
Certain situations require medical evaluation before any rehabilitation movement begins:
- Acute injury with significant swelling — possible ligament rupture, fracture, or dislocation
- Locked joint — inability to fully extend or flex without mechanical blockage
- Severe or worsening pain that prevents weight-bearing
The AAOS recommends immediate medical attention if there is a popping sound with the knee giving way, inability to bear weight, or rapid swelling. These are not Pilates starting points — they're medical situations first.
Severe osteoarthritis with significant structural damage, or rheumatoid arthritis in an active flare, may also require medication management alongside any movement therapy. Johns Hopkins Arthritis Center cautions that too much exercise during an RA flare can increase pain, inflammation, and joint damage.
The Value of Professional Guidance
Even for mild to moderate conditions, one-on-one work with an experienced instructor produces meaningfully different outcomes. What matters is whether the spring tension, range of motion, and alignment cues are appropriate for that person's knee on that specific day.
At The Pilates Room NYC, medical clearance is required before working with injured clients, and instructors are matched to clients based on their specific needs. Several instructors bring credentials directly relevant to rehabilitation:
- Enja Schenck — MS in Sport Science, CSCS certification, trained in Postural Restoration Institute principles
- Ilaria Cavagna — founder of FEET-NESS, a methodology built around posture and foot mechanics
- Pamela Pardi — ELDOA certification alongside 30+ years of classical Pilates experience
That depth of expertise shapes how a session adapts when a client reports more stiffness than usual, or when an exercise that worked last week creates discomfort today.
The studio's no-music, distraction-free environment also supports rehabilitation specifically. When precise alignment and body awareness matter, being able to hear and feel what's happening in your body during movement directly affects how well you progress.
Frequently Asked Questions
Is Pilates good for knee rehabilitation?
Yes. Research and clinical practice consistently back Pilates for knee rehabilitation across conditions including osteoarthritis, patellofemoral pain syndrome, and post-surgical recovery. Its low-impact nature and focus on supporting musculature make it effective at stages where higher-impact exercise isn't appropriate.
What is the best exercise to rehab a knee?
There's no single best exercise. A combination of glute and quad activation (bridge, straight leg raises), hip stabilization (clamshells), and alignment-focused loading (Reformer footwork, assisted squat) — tailored to the rehab phase — consistently outperforms any single movement.
What is the #1 mistake that makes bad knees worse?
Inward knee collapse (valgus) during movement — typically caused by weak hip abductors and external rotators, not the knee itself. Progressing load too quickly before basic alignment and control are established is a close second.
Can I do Pilates after knee replacement surgery?
Yes, gentle Pilates is often recommended after total knee replacement, beginning with Phase 1 exercises like heel slides and clamshells. Get medical clearance from your surgeon or physical therapist first, and work with an instructor experienced in post-surgical rehab.
What Pilates exercises should I avoid with knee pain?
Avoid high-load or complex movements — Russian splits, single-leg parakeet, or deep unsupported lunges — until a diagnosis is established and basic strength and alignment are restored. Stop any exercise that produces sharp pain during or after the session.
How long does it take to see results from Pilates for knee pain?
Most people see reduced pain and improved function within 4–8 weeks of consistent practice. The timeline varies based on the underlying condition, starting strength levels, and whether sessions are instructor-guided or self-directed.