This guide covers both sides: which exercises to avoid and why, and which movements genuinely support hip pain relief. The goal is to help you practice with clarity, not guesswork.
Medical disclaimer: Always consult a healthcare provider before starting or modifying an exercise program, especially if you have a diagnosed hip condition.
Key Takeaways
- Hip pain has multiple causes — OA, tendinopathy, FAI, hip flexor strain — and each responds differently to exercise selection
- Several widely used Pilates exercises (clamshells, sidelying abduction, long-lever leg circles) can aggravate specific hip conditions
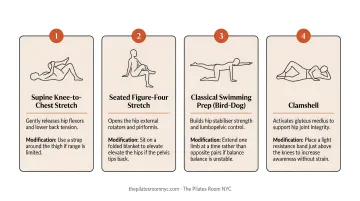
- Bridges, pelvic tilts, modified single-leg circles, and bent knee fall-outs are generally well-tolerated for most hip presentations
- Shortening the lever, reducing range of motion, and prioritizing pelvic stability transforms most exercises into hip-appropriate ones
- Private instruction — not group class programming — is what makes exercise selection genuinely safe for hip conditions
Why Pilates Is a Smart Choice for Hip Pain
Osteoarthritis affects over 32.5 million US adults, and chronic hip pain affects roughly 14.3% of adults over 60. For many of these people, high-impact movement isn't an option — which is exactly where Pilates fits.
Pilates builds strength around the hip joint without placing excessive compressive or shear forces on it. Clinical practice guidelines from JOSPT recommend individualized strengthening, flexibility, and endurance exercise for hip OA — and Pilates, when properly structured, aligns with all three categories.
The Core Stability Connection
One reason hip pain persists is that the muscles meant to stabilize the pelvis (the deep abdominals, pelvic floor, and hip stabilizers) are often underdeveloped. When they underperform, the hip joint compensates, absorbing forces it wasn't designed to handle repeatedly.
Pilates specifically targets this stabilizing chain. Rather than isolating individual muscles, it trains coordinated patterns:
- Pelvis stable and supported throughout movement
- Core engaged before the hip initiates
- Hip moving through a controlled, pain-free range
That combination addresses the actual mechanical problem, not just the symptom.
Flexibility and Stability Together
Passive stretching alone doesn't resolve hip pain. Most people with chronic hip issues have tightness in some structures and weakness in others. Stretching tight muscles without building strength in the weak ones leaves the underlying imbalance intact. Pilates addresses both simultaneously, which is why many physical therapists recommend it alongside PT.
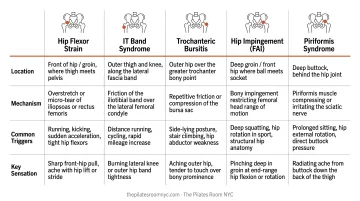
Common Sources of Hip Pain Worth Understanding First
Why Hip Pain Source Determines Exercise Selection
"Hip pain" isn't one condition — it's a spectrum. Exercise selection looks very different depending on what's actually driving the pain.
| Condition | Primary Location | Key Mechanism |
|---|---|---|
| Hip osteoarthritis | Groin, anterior hip | Cartilage degeneration, joint load |
| Hip flexor tightness | Front of hip | Prolonged sitting, muscle shortening |
| Gluteal tendinopathy / GTPS | Lateral hip, greater trochanter | Compressive load on gluteal tendons |
| Hip impingement (FAI) | Groin, deep hip | Abnormal femoral head-acetabular contact |
| Proximal hamstring tendinopathy | Lower buttock, ischium | Compression at ischial attachment |
Where you feel pain tells you a great deal about what's causing it. According to AAFP's classification of adult hip pain, anterior or groin pain typically points to intra-articular pathology (OA, FAI, labral tear) or hip flexor involvement. Lateral hip pain most commonly indicates Greater Trochanteric Pain Syndrome. Posterior pain may involve the hamstring tendons, piriformis, or lumbar referral.
That location tells you something specific: certain movements that are safe for one condition can actively aggravate another. Knowing the source is what makes exercise selection meaningful.
Pilates Exercises to Avoid for Hip Pain
The exercises below are common in general Pilates classes. They're not inherently dangerous, but for people with active hip pain, they place problematic loads on inflamed or sensitive structures.
The Clamshell
The clamshell is widely prescribed for hip pain — often as a first-line glute exercise. The problem: the evidence for its effectiveness is inconsistent, and for certain conditions it's actively contraindicated.
EMG research shows that clamshell activation of the gluteus medius varies considerably. A 2023 study found values ranging from 7.35% to 19.92% MVIC in healthy males — far lower than what's needed to meaningfully strengthen the target muscle. The exercise also tends to recruit the upper gluteus maximus and sartorius via poor lever mechanics.
For anyone with gluteal tendinopathy or Greater Trochanteric Pain Syndrome, the concern is more serious. The clamshell's external rotation and abduction in a compressed sidelying position places provocative compressive load on the greater trochanteric tendons — the very structures that are already irritated. Clinical guidance from JOSPT explicitly advises avoiding hip-adducted postures that increase compressive loading in GTPS.
For most people with lateral hip pain, the clamshell reinforces the irritation — not the stability. A different loading strategy is needed.
Sidelying Hip Abduction
Sidelying hip abduction activates the gluteus medius more effectively than the clamshell — but it comes with its own issues for the hip pain population.
The Tensor Fascia Lata (TFL) is a strong recruiter in this movement, particularly when the leg is positioned in external rotation. For people with hip pain, the TFL is typically already dominant. This exercise can reinforce that dominance while failing to effectively target the deeper gluteal stabilizers that are actually underperforming.
The more pressing concern is what happens at the end of each repetition. When the top leg returns to rest on the bottom leg, the hip moves into adduction — and repetitive hip adduction loading aggravates gluteal tendinopathy, ischiofemoral impingement, and some intra-articular conditions.
In a group class setting, this return phase rarely gets corrected.
Long-Lever Leg Circles and Circumduction
Full leg circles performed with a straight leg (long lever) generate significant rotational and translational forces across the hip joint. For healthy hips with strong local muscular control, this is manageable. For hips dealing with labral pathology, FAI, acetabular dysplasia, or capsular laxity, it can cause excessive shear and abnormal joint contact.
Research on labral tears confirms that repetitive pivoting motions on a loaded femur are associated with acetabular labral damage. Nonoperative FAI management guidelines recommend avoiding movement patterns that provoke impingement at end range.
For those with proximal hamstring tendinopathy, the risk is compounded: high hip flexion with the knee extended compresses the hamstring tendons against the ischium, and adding circumduction introduces friction at an already irritated site.

Pilates Exercises That Support Hip Pain Relief
These movements are generally well-tolerated because they work within a controlled range of motion, prioritize pelvic stability, and load muscles that are commonly weak in people with hip pain — without compressing sensitive structures.
Pelvic Tilts and Pelvic Clock Work
This is the right starting point for nearly any hip presentation. Lying on the back with knees bent, gently rocking the pelvis forward and back — and eventually through small circles — addresses several key needs at once:
- Decompresses the hip joints
- Mobilizes the psoas and deep rotators without loading them
- Re-educates pelvic neutral, which matters for every subsequent movement
- Is appropriate even for significant pain or post-surgical recovery
The pelvic clock, where the pelvis traces a clock face in small gentle movements, adds another dimension of controlled articular mobility without any compressive or shear demand on the hip joint.
Bridges
The bridge is one of the most reliably useful movements for hip pain. It activates both the gluteus maximus and medius in a position that avoids sidelying compression over the greater trochanter, making it preferable to sidelying exercises for anyone with lateral hip pain or gluteal tendinopathy.
Research by Selkowitz et al. confirms that both bilateral and unilateral bridging significantly activate gluteal muscles while minimizing TFL recruitment — exactly the ratio that people with hip pain need.
Modifications are straightforward:
- Feet closer to hips — reduces hamstring demand, easier for anterior hip pain
- Feet farther from hips — increases gluteal emphasis
- Single-leg bridge — only when the double-leg version is pain-free
Modified Single-Leg Circles
Single-leg circles can be hip-appropriate when the key variables are controlled:
- Keep the range small — no full circumduction
- Bend the working knee slightly to shorten the lever
- Hold the pelvis completely still throughout
These adjustments reduce translational forces at the joint significantly. What remains is gentle articular mobilization — enough to improve synovial fluid distribution and maintain hip mobility without provoking labral, capsular, or impingement symptoms.
The pelvis is the non-negotiable variable — if it rocks or rotates to accommodate the moving leg, the exercise has exceeded its appropriate range.
Bent Knee Fall-Out
That same pelvic stability principle carries into the bent knee fall-out — a gentle way to address hip rotator tightness and hip flexor tension. Lying on the back with knees bent and feet flat, one knee slowly drops outward as far as it will go without the pelvis shifting, then returns.
This movement provides traction and mobility to the deep rotators without compression. NHS Inform includes it in their recommended exercises for hip osteoarthritis, and it's particularly useful before loading for anyone with early-stage OA stiffness or hip flexor tightness.
Modifications and the Value of Personalized Instruction
Three adjustments transform almost any Pilates exercise into a hip-appropriate one:
- Shorten the lever — bend the knee rather than working with a straight leg
- Reduce range of motion — work within a pain-free zone, not to end range
- Prioritize pelvic stability — no hip mobility work should occur at the cost of pelvis movement
Mat vs. Reformer for Hip Pain
For people with significant hip pain, the Reformer often has genuine advantages over mat work. Spring assistance allows the limbs to move with support rather than fighting gravity alone — which means range of motion can be controlled precisely, and movements that would be provocative on the mat can be performed safely on the Reformer at appropriate spring settings.
That said, the Reformer is only more accommodating when programmed correctly for the individual. An exercise performed on the Reformer with too large a range or poor spring selection can be just as problematic as the mat equivalent.
When to Stop and Modify
There's a meaningful difference between muscular effort and joint irritation. Stop or modify any exercise that causes:
- Pinching or catching in the groin or deep hip
- Sharp lateral hip pain during or after the movement
- Pain that persists beyond the session itself
Mild muscular fatigue during a well-designed session is expected. Pain that lingers is a signal worth taking seriously.
Working with a Knowledgeable Instructor
Generic class programming can't account for individual hip presentations. At The Pilates Room NYC in Chelsea, instructors with backgrounds in sport science, strength and conditioning, and postural restoration assess each client's specific condition and adapt classical Pilates programming accordingly.
Private sessions provide access to the full classical apparatus — Reformer, Tower, Cadillac, Wunda Chair, and mat — with exercise selection and range of motion adjusted to each person's pain presentation and recovery stage rather than following a standardized sequence.
Frequently Asked Questions
Should you do Pilates with hip pain?
Yes — Pilates is appropriate for most hip pain when properly modified. It's low-impact, builds supportive musculature, and aligns with clinical guidelines for conditions like hip OA. Exercise selection and range of motion must be adjusted to the specific condition, ideally with a rehabilitation-experienced instructor guiding the process.
What causes hip pain during Pilates?
Most often: too large a range of motion, exercises that place compressive load on irritated tendons or joints (clamshells and long-lever circles being common culprits), or poor pelvic alignment that transfers force to the hip. Each of these issues responds well to targeted modifications once identified.
Is Reformer or mat Pilates better for hip pain?
For significant hip pain, the Reformer often has an advantage because spring assistance allows supported, controlled movement within a comfortable range. Both formats can be effective when exercises are appropriately selected — the equipment matters less than the programming.
Can Pilates help with hip pain from arthritis?
Research supports exercise as beneficial for hip osteoarthritis, and Pilates aligns with clinical guidelines recommending individualized strengthening and mobility work. Avoiding high-load or high-impact movements and staying within a pain-free range are essential — a certified instructor can structure appropriate progression from there.
How long does it take to see improvement in hip pain with Pilates?
Clinical exercise programs for hip OA commonly use 6–12 week dosing windows, and many people notice reduced stiffness and improved mobility within several weeks of consistent, properly modified practice. Results vary by condition severity and session frequency.
When should I stop Pilates and see a doctor about hip pain?
Seek medical evaluation if hip pain is sudden or severe, follows a fall or injury, or if you experience joint locking, giving way, or groin pain radiating down the leg. Also consult a provider if pain consistently worsens after sessions — these may indicate conditions that need assessment before continuing exercise.