Introduction
According to the American Association of Neurological Surgeons, scoliosis affects an estimated 6 to 9 million people in the United States — roughly 2 to 3% of the population. Most cases are first identified between ages 10 and 18, making it one of the most common musculoskeletal conditions affecting adolescents. For many, a diagnosis arrives and then sits unanswered: what now?
Living with scoliosis means managing more than a curved spine. The lateral deviation and vertebral rotation create asymmetrical muscle use on both sides of the body — one side shortened and overworked, the other elongated and underused. Over time, those compensations compound into chronic stiffness, fatigue, and pain.
Those exact imbalances — tight muscles, underactive stabilizers, restricted breath — are where Pilates excels. Its spine-centered focus, controlled progressions, and emphasis on core stability align directly with what a scoliotic body needs. But safe practice requires knowing which exercises help, which to modify, and why individualized guidance matters.
Key Takeaways
- Pilates cannot structurally correct scoliosis, but consistent guided practice can reduce pain, improve posture, and strengthen spinal stabilizers
- Effective scoliosis Pilates prioritizes axial elongation, breath work, and bilateral muscular balance over aggressive stretching
- Some movements (end-range rotation, deep loaded flexion) can worsen symptoms and need modification
- No two curves are alike — safe programming must match the individual's specific curve type, severity, and pain levels
- Medical clearance from a physician or spine specialist is essential before starting, especially for curves above 25–30 degrees
What Scoliosis Does to Your Spine — and Why Pilates Is a Natural Fit
Scoliosis Is a 3-Dimensional Problem
Scoliosis is more than a sideways bend. Clinically defined as a lateral spinal curve measuring more than 10 degrees — but that description understates what's actually happening. Peer-reviewed literature published in PMC describes scoliosis as a multifactorial 3D spinal deformity involving lateral curvature, vertebral rotation, and deviations in multiple planes simultaneously.
This distinguishes it from the spine's normal curves — cervical lordosis, thoracic kyphosis, and lumbar lordosis — which are front-to-back and exist in a single plane. Scoliosis curves often appear as a "C" or "S" shape on X-ray and may involve the thoracic region, lumbar region, or both.
Understanding this 3D nature matters for exercise selection. An intervention that addresses lateral deviation without accounting for vertebral rotation misses a significant part of the picture.
The Muscular Compensation Cascade
Scoliosis reshapes the soft tissue around the spine, not just the bones. Research supports that it creates asymmetric muscle activation and asymmetric weakness, though the pattern varies by individual and curve type.
The concave (inner) side of the curve tends to become shortened and overactive; the convex (outer) side becomes elongated and relatively weaker. This imbalanced tissue development leads to:
- Fatigue on the overloaded side
- Reduced mobility through the stiffened areas
- Compensatory movement patterns in the hips, shoulders, and ribcage
- Chronic discomfort that worsens with gravitational load over time
No two curves produce identical compensations. A right thoracic curve creates a different muscular picture than a left lumbar or combined S-curve. Curve type and location must therefore drive every exercise decision.
Why Pilates Fits
Pilates is spine-centered by design. Its core principles — controlled movement, axial length, diaphragmatic breath, and muscular balance built from the center outward — address the exact biomechanical challenges scoliosis creates.
Specifically, Pilates offers:
- Core strengthening without axial compression — essential for a spine already under asymmetric load
- Segmental spinal mobility work — addressing stiffness at the curve's apex
- Breath integration — a functional tool for mobilizing the compressed, concave ribcage
- Individualized programming — adaptable to each client's curve type and presentation
A 2021 meta-analysis of 10 randomized controlled trials found that Pilates exercise training may improve Cobb angle, trunk rotation, pain, and quality of life in people with scoliosis. The evidence is promising, though researchers note that more high-quality studies are needed. What the data supports is this: Pilates adapted to the individual's specific curve has a meaningful role in long-term scoliosis management.
Safe Pilates Exercises for Scoliosis
The exercises below are generally considered appropriate for mild to moderate idiopathic scoliosis. All should be performed under the guidance of a qualified instructor before being attempted independently. What works well for one curve may be contraindicated for another.
More important than Cat-Cow itself is the underlying principle it embodies: axial elongation. The conscious act of lengthening the spine upward against gravity is the most important concept in all scoliosis Pilates work.
It reduces multi-plane compression in the curve's concavities and encourages the nervous system to find better alignment patterns before any load or range of motion is added. Every exercise — from supine to seated to standing — should begin from a sense of length through the spine.
Breath Work as an Active Tool
Directed breath is not just a relaxation cue — it's a functional intervention for scoliosis. Scoliosis-specific exercise literature describes the value of guiding inhalation into the collapsed, concave side of the ribcage to:
- Gently mobilize the ribs on the restricted side
- Create space between spinal segments
- Counteract the compression gravity constantly imposes on the concavities
This technique is much more effective with hands-on or tactile cueing from a trained instructor. Feeling the breath expand into the right area is difficult to achieve from verbal instruction alone, particularly early in the process.
How to Practice Pilates Safely When You Have Scoliosis
Get Medical Clearance First
Before beginning any Pilates program, consult a physician or orthopedic spine specialist — particularly if you have:
- A Cobb angle near or above 25–30 degrees
- Active pain or neurological symptoms
- A history of spinal fusion surgery
- Neuromuscular scoliosis
- Rapidly changing posture
At The Pilates Room NYC, the studio's health policy aligns with this approach: doctor clearance is required for clients with relevant health conditions before beginning sessions. If you've received that clearance, instructors design programming specifically around your condition.
Work with a Qualified Instructor
Scoliosis is highly individualized. The same exercise can be beneficial for one curve type and harmful for another : a lateral bend performed on the wrong side can reinforce existing imbalances rather than correct them. Look for an instructor with specific training or meaningful experience working with scoliosis clients.
At The Pilates Room NYC, senior instructors bring 15 to 35 years of teaching experience and specialized expertise in scoliosis support. Enja Schenck (MS in Sport Science, CSCS) integrates Postural Restoration Institute principles — focused on posture and asymmetry management — into her classical Pilates teaching, making her particularly well-suited for clients with spinal asymmetries. For anyone with scoliosis, private or semi-private sessions are the safest starting point.
Start with a Movement Assessment
A qualified instructor should begin with a structured movement assessment before any exercise begins. That typically means:
- Observing posture and identifying the curve's direction and approximate location
- Assessing where mobility is restricted versus excessive
- Noting compensatory patterns in the hips, shoulders, and ribcage
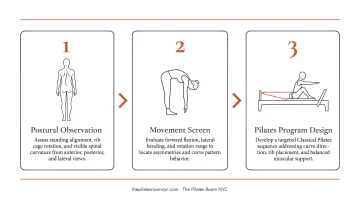
This assessment shapes everything that follows: which exercises to include, which to modify, and which to avoid entirely.
Prioritize Neutral Spine Over Forced Correction
The most effective position for neuromuscular re-patterning in scoliosis is a supported, neutral spine. Exercises performed lying down, on the side, or in positions that reduce gravitational load allow the nervous system to begin learning more balanced movement patterns before progressing to standing or loaded work.
Trying to aggressively correct the curve through exercise — rather than working patiently from a supported, elongated position — often backfires.
Movements and Approaches to Modify with Scoliosis
Deep Flexion Combined with Rotation
Exercises that combine deep forward bending with simultaneous rotation — like unsupported roll-downs or twisting sit-up variations — can increase compression on vertebral segments that are already under asymmetric load. This doesn't mean all rotation is off-limits. The concern is end-range, loaded, or unsupported rotational movements, particularly when performed without an instructor present to observe and adjust.
One-Size-Fits-All Programming
Applying a generic Pilates sequence to a scoliosis client is one of the most common — and most consequential — mistakes. A side plank or lateral bend performed on the wrong side can reinforce the existing imbalance. Exercises must be selected based on the individual's specific curve type, direction, and location.
That specificity is what separates a well-designed scoliosis program from one that accidentally works against the spine it's meant to support.
High-Load Spinal Work Without a Foundation
Even the right exercises become problematic at the wrong intensity. Movements with significant axial compression — heavy loading, vigorous impact, or advanced repertoire before core stability is established — can aggravate scoliosis, particularly in adults with degenerative curves or reduced bone density.
Watch for these high-load scenarios that warrant extra caution:
- Advanced Pilates repertoire attempted before a stable baseline is in place
- Weighted or resistance-loaded spinal movements without instructor supervision
- Impact-based exercise (jumping, dynamic transitions) on a spine that hasn't been assessed for tolerance
- Rapid progression driven by motivation rather than how the body responds session to session
How Often to Practice and What to Realistically Expect
Frequency
Research on scoliosis-specific exercise programs offers a useful benchmark. Studies have used structured programs of approximately:
- 27 sessions over 3 months — with observed improvements in flexibility and pain reduction
- 12 weeks of supervised Pilates-based programs — with Cobb angle improvements in adolescents
- 24 weeks of combined Schroth-Pilates programming — with improvements in Cobb angle, trunk rotation, chest expansion, and quality of life
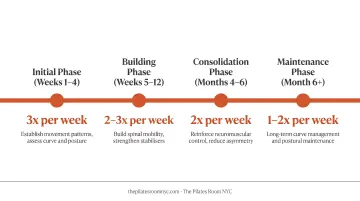
Based on this, 2 to 3 sessions per week is a reasonable general guideline, but the right frequency for any individual depends on curve severity, pain levels, age, and input from both a healthcare provider and a qualified instructor. Irregular practice tends to undo cumulative postural gains — which is why showing up regularly, even briefly, matters more than occasional intense effort.
Realistic Expectations
Pilates is a management strategy, not a cure. Results to realistically expect with consistent, well-guided practice include:
- Reduced pain and daily discomfort over weeks to months
- Improved awareness of where the body is in space and how it moves
- More balanced musculature across the trunk and back
- Greater ease with sustained sitting, standing, and everyday movement
Structural spinal curves will not disappear. Gains develop gradually and require ongoing practice to maintain. For most people, meaningful change becomes noticeable across months — and holding those gains means continuing to practice beyond the point when things start to feel better.
Frequently Asked Questions
Does Pilates help with scoliosis?
Pilates cannot structurally correct scoliosis, but it is well-supported as a management approach. Research suggests it may improve postural alignment, reduce pain, strengthen spinal stabilizers, and support quality of life — particularly with consistent, properly guided practice adapted to the individual's curve.
Which is better for scoliosis, Pilates or yoga?
Pilates has a clear advantage for scoliosis due to its spine-centered focus and an instructor's ability to tailor sessions to your specific curve type and direction. Yoga classes are generally less individually adapted — a real limitation when the same pose affects a right thoracic and left lumbar curve very differently.
What should I avoid in Pilates if I have scoliosis?
Approach with caution: unsupported deep spinal flexion combined with rotation, exercises applied without curve-specific modifications, and loaded or end-range spinal movements performed without qualified supervision. Movement is not the enemy — working without proper guidance is.
Can Pilates straighten or correct a scoliotic curve?
Pilates cannot reverse a structural spinal curve. It can improve postural alignment and reduce the functional impact of the curve. In adolescents whose bones are still developing, it may also support slowing progression when combined with medical management.
How often should I do Pilates for scoliosis?
Two to three sessions per week is a reasonable general guideline, based on research program structures. Individual frequency should be adjusted based on severity, pain levels, and guidance from both your healthcare provider and a qualified Pilates instructor.
Do I need private sessions for scoliosis, or can I join group classes?
Private or semi-private sessions are strongly recommended at the start — scoliosis requires individualized exercise selection and cueing that group classes cannot reliably provide. Once a safe, personalized routine is established, some individuals can transition to small group settings with the right modifications in place.