The problem with that? Standard fitness advice — stretch more, build flexibility, push your range — can actively make things worse for hypermobile bodies. What feels like a productive workout can quietly erode joint stability, trigger pain flares, and reinforce compensatory movement patterns that cause cumulative harm.
This guide covers what hypermobility actually means for movement, the core principles that make Pilates safe and effective for this condition, which exercises build the stability hypermobile joints need, and the mistakes that most commonly cause setbacks.
Key Takeaways
- Hypermobility is a joint stability problem, not a flexibility problem — and Pilates addresses it directly by training deep stabilizing muscles
- Safe Pilates for hypermobility means working within a controlled mid-range, not chasing full range of motion
- Exercises like Dead Bug, Bridging, and Quadruped build the active muscular support that lax ligaments cannot provide
- Overstretching, hyperextending joints, and rigid core bracing are the most common mistakes hypermobile people make — and the most damaging
- Starting with private, 1:1 instruction before joining group classes is strongly recommended for this population
What Hypermobility Actually Means for Movement
It's a Connective Tissue Issue, Not Just Flexibility
Joint hypermobility means joints move beyond the typical range of motion due to differences in connective tissue structure — not simply being "bendy." This exists on a spectrum: from benign joint hypermobility with minimal symptoms, to Hypermobility Spectrum Disorders (HSD), to hypermobile Ehlers-Danlos Syndrome (hEDS), a clinical diagnosis requiring generalized joint hypermobility plus systemic features and exclusion of other conditions.
When ligaments are lax, the deep stabilizing muscles must carry the load of keeping joints safe and supported. In most hypermobile people, those muscles are undertrained. The body compensates by recruiting the wrong muscles — gripping quads, overworking upper traps, tensing the jaw — creating patterns that feel stable but aren't.
A 2022 systematic review found that hypermobile adults show partially impaired lateral abdominal muscle function, specifically a reduced ability to increase transversus abdominis thickness during contraction. One of the primary deep stabilizers is already at a disadvantage before any exercise begins.
The Anxiety-Hypermobility Connection
Research consistently links hypermobility to elevated anxiety rates, likely tied to autonomic nervous system reactivity. Movements that demand breath-holding, increase nervous system arousal, or create unpredictable joint sensations can worsen both physical symptoms and psychological stress responses — which makes exercise selection especially consequential for this population.
A 2025 study also found poorer elbow and knee proprioception in hypermobile adults — meaning the body's ability to sense where joints are in space is compromised. Since lax ligaments don't provide normal sensory feedback to the brain, hypermobile people often can't reliably detect when they're in a dangerous position until something hurts.
Why Standard Exercise Often Backfires
Group fitness classes, yoga, and even standard Pilates can be counterproductive when they:
- Encourage end-range flexibility or passive stretching
- Include unsupported inversions or rapid position changes
- Reward range of motion over control
- Apply rigid "brace your core" cues without individualized assessment
The problem is exercise that prioritizes the wrong qualities for this population.
Safe Pilates Principles for Hypermobile Bodies
The goal of Pilates for hypermobility is not to increase flexibility. It's to build active joint stability — training muscles to hold each joint in its optimal position throughout movement.
Stability Before Strength, Strength Before Endurance
The progression matters: establish deep stabilizer activation first (transversus abdominis, pelvic floor, multifidus), then layer in strength with controlled load, then add endurance or complexity. Skipping this sequence is a primary cause of flares and injury in hypermobile clients.
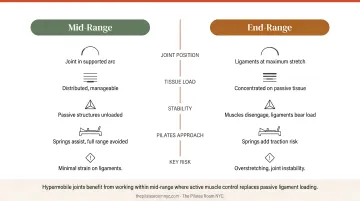
Joint Centration and Mid-Range Work
Guiding each joint into its most mechanically supported position before adding load or movement is essential. Without this, hypermobile joints rely on passive structures (already lax ligaments) rather than active muscular support.
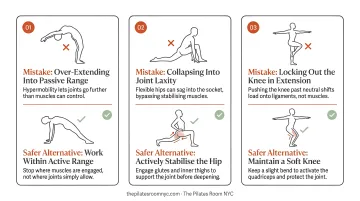
A practical example: keeping a soft micro-bend in elbows and knees rather than locking them out. Locked joints feel stable to hypermobile people because they require less muscular effort. But they're actually hanging on passive structures, accumulating strain with every repetition.
Working within a reduced, controlled range of motion — not the full range a hypermobile body can achieve — is safer and more therapeutic. The end range is where hypermobile joints are most vulnerable. Strength built in mid-range transfers more safely to daily function.
Breath as Regulation, Not Bracing
The "navel-to-spine" bracing cue common in many Pilates classes can create unhelpful over-recruitment patterns, interfere with breathing mechanics, and place excess load on the pelvic floor. For hypermobile clients, rigid bracing tends to increase overall body tension without actually improving joint stability.
Breath-led movement that stays relaxed, rhythmic, and linked to effort supports both stability and nervous system calming — and it changes how the entire session feels for a hypermobile body.
Proprioception as a Priority
Because lax ligaments don't provide normal sensory feedback, proprioception training is central to any hypermobility program. Pilates addresses this through:
- Slow, intentional movements that demand body awareness
- Tactile feedback (hands on a mat, feet pressing into a footbar)
- Closed-chain exercises that load through the limb into a fixed surface
- Classical apparatus (Reformer, Cadillac, Wunda Chair) that provides spring resistance as external proprioceptive input
Pilates Exercises That Build Stability for Hypermobility
The exercises below target core control, stabilization, and proprioception. All require instructor guidance to be safe and effective for hypermobile bodies — the same movement can be therapeutic or harmful depending on how it's cued and how much range is used.
Dead Bug
Lying on your back with arms and legs raised, you alternately lower opposite arm and leg while keeping the spine and pelvis completely still. The floor provides constant tactile feedback, which helps hypermobile clients build body awareness in a supported position — without loading the spine.
Key modification: Keep the range small. The lower back stays in contact with the mat throughout. If the back arches as the limbs lower, bring the range back in.
Bridging
Lying on your back with feet flat, you lift the pelvis off the floor in a slow, segmental movement. This strengthens the glutes and hamstrings — both typically underactive in hypermobile bodies — and trains the pelvis to move with intention rather than momentum.
Key modification: Stop short of full height. The goal is a straight line from shoulders to knees, not an arch. The moment the lower back begins to compress, that's the ceiling.
Quadruped (Bird Dog)
On hands and knees, you extend the opposite arm and leg while holding the spine completely neutral. Floor contact under hands and knees provides grounding feedback, making this one of the most effective anti-rotation exercises for hypermobile clients.
Key modification: Wrists directly under shoulders, elbows soft — not locked. Move the limbs only as far as the spine stays still. If the lower back rotates to follow the arm, bring the range back in.
Chest Lift
What it is: A controlled spinal flexion exercise performed on the back, lifting only the head and shoulders off the mat with hands supporting behind the head.
Why it works: Trains the anterior chain without loading the cervical spine unsupported. The small range keeps the work in the safe mid-range for a hypermobile spine — away from the end-range positions where instability is greatest.

The mat exercises above build a foundation of body awareness and core control. When working on the Reformer, that same awareness translates to apparatus — with the added benefit of spring resistance as a proprioceptive tool.
Footwork on the Reformer
Pressing the carriage out and in through the feet against spring resistance, with the spine fully supported on the headrest. The springs provide feedback through the entire range of motion, and the footbar creates a physical stop that prevents knee hyperextension — something hypermobile clients often default to.
Start with soft spring resistance. Prioritize feeling the muscles work over achieving full carriage travel.
How to Start Pilates Safely When You're Hypermobile
Begin with Private Instruction
Starting with a private, 1:1 session (rather than a group class) gives an instructor the opportunity to observe how you actually move: where you default to hyperextension, which stabilizers are underactive, and what compensatory patterns are already in place. This assessment shapes the entire program that follows.
At The Pilates Room NYC in Chelsea, Manhattan, hypermobility is explicitly listed as a condition supported through private sessions. Instructors work with a client-centered approach that tailors each session to the individual's physical state. The studio also offers apprentice-level sessions at $80 per session for clients who want qualified, supervised instruction at a more accessible price point.
For clients whose needs require a more specialized lens, instructors like Enja Schenck — holding an MS in Sport Science, CSCS certification, and training in Postural Restoration Institute methodology — bring a particularly relevant skill set for joint stability and postural compensation work.
What to Tell Your Instructor
Before your first session:
- Disclose your hypermobility diagnosis, or suspected hypermobility, in the intake form
- Ask whether the instructor has experience with hypermobility or connective tissue disorders
- Clarify that your goal is stability, not flexibility
- Mention any comorbidities — particularly POTS or orthostatic symptoms, which directly shape exercise selection
Group mat classes are best delayed until a foundation of stability has been established in private sessions.
Pacing and Fatigue Management
How your body responds between sessions matters as much as what happens during them. Research shows that individuals with joint hypermobility syndrome experience greater delayed-onset muscle soreness and need more recovery time after strenuous exercise. Track how you feel in the 24-48 hours after each session — that window tells you whether your load is calibrated correctly.
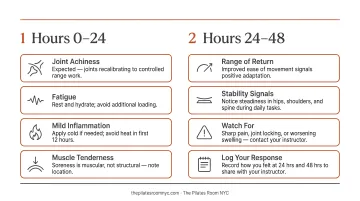
Signs to reduce load (not push through):
- Increased joint pain or swelling the following day
- Unusual fatigue that disrupts daily function
- Flare-ups of existing symptoms
Consistency over time produces better long-term outcomes than intensity followed by recovery days. Shorter, more moderate sessions done regularly outperform ambitious sessions with long gaps between them.
Common Mistakes Hypermobile People Make in Pilates
Treating Tightness as a Flexibility Problem
Many hypermobile people feel chronically tight — but this tightness is often protective muscle tension compensating for unstable joints, not true muscle shortness. Stretching these areas removes the body's last line of defense against instability.
The EDS Society notes that while gentle muscle stretching can help when muscles are genuinely tight, overstretching beyond normal range can be harmful. For hypermobile people, Pilates should be a stability practice first — flexibility is already there.
Hyperextending Joints Under Load
Hypermobile clients naturally drift into end-range positions — locked knees in standing, hyperextended elbows in plank — because these positions require less muscular effort. They feel stable. They're not.
These positions load passive structures: ligaments, joint capsules, tendons. Cumulative strain in these tissues increases injury risk and slows recovery time.
Rigid Core Bracing
The "hollow and brace" cue can create excessive tension, interfere with breathing, and overload the pelvic floor. For hypermobile clients specifically, it tends to increase global body tension without actually improving joint stability.
Functional, breath-linked engagement — where the core responds to movement rather than bracing ahead of it — is both more effective and more sustainable.
Ignoring Pacing
The pattern is common: a hypermobile client feels good in a session, does more than planned, and experiences a significant crash or flare 24–36 hours later. Repeat this enough times and the cycle itself becomes a barrier to progress.
Pacing belongs in the program design from day one, not added as an afterthought when something goes wrong.
Frequently Asked Questions
Which is better for hypermobility, Pilates or yoga?
Modified Pilates is particularly well-suited for hypermobility because it emphasizes stability, controlled loading, and proprioception. Many yoga styles encourage end-range flexibility and passive stretching, which can worsen hypermobile joint instability. Yoga can be adapted, but requires the same careful approach as modified Pilates.
Is Reformer Pilates safe for hypermobility?
Yes — when introduced gradually with a qualified instructor. Reformer spring resistance provides proprioceptive feedback, the equipment creates natural limits on range of motion, and the supported positions help clients find stable alignment. Soft spring settings and close instructor supervision are especially important early on.
What Pilates exercises should hypermobile people avoid?
Approach with caution: unsupported inversions (particularly with POTS or neck instability), roll-overs that load the cervical spine, and any weight-bearing exercise performed in hyperextended joint positions. In practice, this means finding a stable mid-range position rather than eliminating the movement altogether.
Can Pilates help with Ehlers-Danlos Syndrome (EDS)?
Yes. The NHS lists Pilates as a lower-risk activity for people with EDS, and EDS UK supports modified basic mat Pilates for core strength, proprioception, body awareness, and posture. Clinical and specialist instructors experienced in hEDS can design programs that build stability without triggering flares.
How often should someone with hypermobility do Pilates?
Start conservatively and track how your body responds in the 24–48 hours after each session. Consistency matters more than frequency or intensity. Even short daily movement sessions work well alongside less frequent structured Pilates work.
Should I tell my Pilates instructor I'm hypermobile?
Yes — always disclose before your first session. It allows the instructor to identify compensatory movement patterns, adjust cues, and avoid triggers like end-range loading or rigid bracing. An instructor unfamiliar with hypermobility should be willing to learn or connect you with a more specialized colleague.