The Pilates reformer has become a go-to tool across this entire spectrum, from acute pain management to return-to-sport conditioning. Its spring-based resistance system lets you load the muscles around the knee without the compressive forces that make exercises like lunges or squats unbearable when pain is present.
That said, results depend on more than just showing up. The right exercises, appropriate spring tension, clean alignment, and a qualified instructor who understands the full movement chain—these are what separate genuine progress from frustration. This article covers all of it.
Key Takeaways
- Horizontal resistance on the reformer significantly reduces the compressive load on the knee joint
- Strengthening hips, glutes, and core matters as much as targeting quads and hamstrings
- Spring tension, range of motion, and hip-knee alignment are the three variables that most directly shape results
- Working with a qualified instructor—not just following a generic exercise list—is essential for safe, lasting results
Why the Reformer Works for Knee Pain
The Mechanics of Spring Resistance
On a standard reformer, the carriage moves horizontally. Your body weight is supported by the carriage, so the knee isn't bearing a vertical load the way it does during a squat or lunge. This matters because patellofemoral joint stress increases substantially with knee flexion angle—activities requiring deep knee bend expose the joint to far greater forces than those performed in a smaller range.
The reformer lets you work in that smaller, safer range while still challenging the muscles that protect the joint. Strength builds first; range of motion follows, without the pain spikes that come from pushing too far too soon.
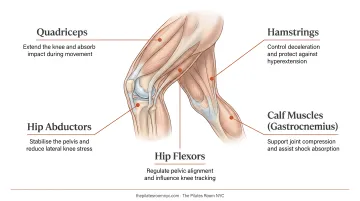
The Muscles That Actually Protect Your Knee
Most people focus on the quads, but knee stability depends on a network of muscles that extends well beyond the joint itself:
- Vastus medialis oblique (VMO) — the teardrop-shaped quad muscle near the inner knee; delayed VMO activation correlates with patellar maltracking in patellofemoral pain
- Medial hamstrings — the semitendinosus and semimembranosus control tibial rotation during knee extension, which directly affects joint mechanics
- Glute medius and hip abductors — weakness here increases hip adduction and internal rotation, creating a chain reaction that stresses the patellofemoral joint
- Gastrocnemius — calf tension affects both ankle mechanics and the forces transmitted through the knee during loaded movement
- Ankle dorsiflexors — reduced ankle dorsiflexion is significantly associated with dynamic knee valgus, meaning a stiff ankle can drive the knee inward under load
The reformer, unlike an isolated leg extension machine, can address all of these in a single session. An instructor can shift from footwork targeting the VMO to leg circles improving hip mobility to standing exercises loading the glute medius—without the client ever moving off the equipment.
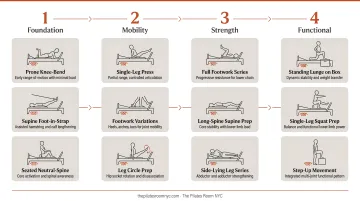
A Tool for Every Stage of Rehab
The reformer's range is what makes it genuinely useful across the entire rehab arc—not just the early stages. Spring resistance starts light for acute pain management and increases as strength returns. Body position shifts to match each phase of recovery:
- Supine (lying down) — foundational work with minimal joint load; appropriate for acute pain or early post-PT
- Seated — midstage loading that introduces more functional demand on the knee
- Standing — return-to-function work that mirrors the demands of walking, stairs, and daily movement
One piece of equipment, used well, covers all three.
Best Reformer Pilates Exercises for Knee Pain
These exercises progress from foundational (low joint demand) to functional (weight-bearing). Spring settings should always be confirmed with an instructor based on your specific pain level and strength—there are no universal prescriptions.
Footwork: Heels, Parallel, and Pilates V
Setup: Lie supine on the carriage with feet on the footbar. Press through the heels to extend the legs, then control the return.
This is the first exercise prescribed in most knee rehab progressions because body weight is fully supported. The emphasis on achieving full knee extension—not a "soft knee"—activates the VMO and establishes correct patellar tracking patterns from session one.
Watch for:
- Knees tracking in line with the second toe throughout the movement
- Any inward collapse during extension, which signals a hip stability issue to address before increasing load
Spring guidance: Start with moderate resistance and reduce immediately if there's any pain at end-range extension. Your instructor should be watching alignment, not just counting reps.
Leg Circles in Straps
Setup: Supine with both feet in the straps, performing controlled circular movements originating from the hip.
The purpose here isn't hip flexibility—it's hip-knee dissociation. Many people with knee pain have learned to generate rotation through the knee rather than the hip. This exercise teaches the correct pattern: rotation comes from the ball-and-socket joint, not the hinge joint.
Watch for: Keep the pelvis completely still. If it rocks, the circle is too large. A controlled range reduces shear forces on the medial and lateral knee structures.
Short Spine Massage
Setup: Feet in straps, draw knees toward the chest, curl the spine up and over, then roll down sequentially.
This builds posterior chain strength—hamstrings and glutes—in a fully supported, decompressed position. There is zero compressive load on the knee, making it valuable even for clients with significant pain.
For knee flexion pain: Limit how deeply the knees bend on the return phase by stopping earlier in the range or adjusting spring length. An instructor can identify exactly where pain begins and keep movement below that threshold.
Scooter (Single-Leg Standing on Carriage)
Setup: One foot on the stationary footbar, the other foot on the carriage, pressing back into a single-leg stance.
This is a progression exercise, introduced only after footwork is pain-free and hip alignment is solid. It's a closed kinetic chain movement that directly trains the hip stability and landing mechanics needed for real-world activities—stairs, walking, gentle sport.
Watch for: Full hip and knee extension at the end of each push to activate the VMO. Without this, the exercise becomes a momentum drill rather than a strengthening one.
Assisted Squat / Leg Press
Setup: Standing or seated, using spring assistance to reduce the load the knee must manage through the squat pattern.
This bridges the gap between mat-based exercises and the functional movements knee pain most commonly disrupts: standing from a chair, descending stairs, getting in and out of a car.
Watch for: Press evenly through both feet, knees tracking over the second toe, and no excessive forward travel of the knee over the toes. Spring assistance reduces incrementally as strength and confidence build—most clients feel the clearest connection between reformer work and daily function here.
Key Variables That Affect Your Results
How you manage these four variables session to session will determine whether your knee responds well or stalls out.
Spring Tension
Too little resistance provides insufficient muscular stimulus. Too much creates compressive forces that aggravate inflamed or arthritic tissue. The right starting point is moderate resistance that challenges the muscles without triggering pain during or after the session.
Progress is guided by response, not a fixed schedule. If pain increases noticeably the morning after a session, the load was too high.
Research on therapeutic exercise progression supports using 24–48 hour post-exercise checks for soreness and stiffness as a standard monitoring tool. If symptoms subside overnight and don't accumulate week over week, you're in a workable range.
Range of Motion
Deep knee flexion past 90–120 degrees increases patellofemoral joint stress considerably. Working in a pain-free, partial range allows the muscles to be loaded and strengthened without aggravating the joint surface.
Clients who attempt full range of motion before building sufficient strength are the most likely to experience flare-ups. Train at the edge of your pain-free range, build strength there, and let the range expand as a result. Forcing range before strength is in place tends to set recovery back.
Hip and Knee Alignment
Dynamic knee valgus (knees caving inward during loaded movement) is one of the most consistently harmful patterns in knee rehabilitation. Research confirms that valgus kinematics correlate with task-elicited pain in patellofemoral pain syndrome, and that the pattern also stresses ACL mechanics.
Verbal and tactile cueing from the instructor to maintain hip-knee-foot alignment during every repetition is more important than the number of reps completed. Consistent alignment cues protect the joint far more than adding volume.
Consistency and Progression Timeline
Knee rehabilitation requires neuromuscular re-education: the timing patterns of the VMO and glute medius need to be retrained through consistent repetition over weeks, not just loaded harder.
Research supports three or more exercise therapy sessions per week as more effective for hip and knee conditions than fewer than two sessions per week. Two to three sessions weekly is a practical target for most people managing knee pain.
Who Should (and Shouldn't) Try Reformer Pilates for Knee Pain
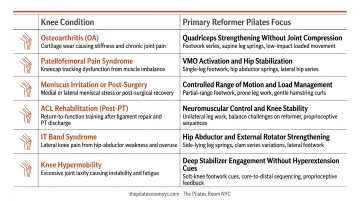
Conditions That Typically Respond Well
The reformer is widely used across a range of knee conditions, though each requires a different exercise emphasis:
- Patellofemoral pain syndrome (runner's knee) — VMO activation, hip stability, and controlled range of motion are the primary targets
- Knee osteoarthritis — low-load strengthening and neuromuscular training; a 2025 systematic review found Pilates-based exercise produced pain reduction versus no intervention
- Post-surgical rehabilitation — ACL repair, meniscus surgery, and knee replacement (with physician clearance) all benefit from the supported, graduated loading the reformer provides
- IT band syndrome — hip abductor and TFL work to address the proximal cause of lateral knee irritation
- General muscle imbalances — often the underlying driver of chronic knee pain without a specific diagnosis
When to Get Medical Clearance First
Reformer Pilates is not appropriate as a first response to:
- Recent fractures or acute severe swelling
- Undiagnosed knee pain (get a diagnosis before starting any exercise program)
- Suspected deep vein thrombosis (DVT)
- Pain that worsens with any movement whatsoever
A physician or physiotherapist should provide clearance before starting a reformer program if any of these apply. The studio works with post-clearance clients—not instead of medical care.
Working with Experienced Instructors
At The Pilates Room NYC, the instructor team brings substantial rehabilitation experience to knee-related work:
- Enja Schenck (MS in Sport Science, CSCS) integrates Postural Restoration Institute principles with classical Pilates and strength and conditioning — a combination well-suited to rehabilitation
- Alison Johnson, studio owner, brings 26 years of teaching across injury recovery, post-surgical rehab, and diverse client populations
- Pamela Pardi has over 30 years in the classical tradition, with experience guiding clients through chronic pain and post-op recovery
Each session is adapted to the client's physical state that day, which matters when pain levels shift week to week. Private sessions are the recommended format for knee rehabilitation, as they allow full customization of spring tension, range of motion, and progression without the constraints of a group setting.
Common Mistakes That Make Knee Pain Worse
Three patterns come up repeatedly in clients managing knee pain on the reformer. Recognizing them early prevents setbacks.
- Valgus collapse during footwork or squats. Knees caving inward stresses the patellofemoral joint and disrupts patellar tracking — the pattern most likely to cause or worsen pain, even at light spring resistance. Hip stability work needs to come first.
- Progressing too quickly. Adding spring tension or range of motion before the current load feels stable almost always triggers flare-ups. If pain increases the morning after a session, that's a signal to reduce load — not push through.
- Isolating the knee while ignoring hip and ankle. Quad strengthening alone leaves the root mechanical causes unaddressed. Symptoms return even after strength improves because the underlying movement patterns haven't changed.
Avoiding these patterns is what separates sessions that build resilience from ones that set recovery back.
Frequently Asked Questions
Is Reformer Pilates good for knee pain?
Yes. The reformer's spring-based resistance reduces compressive joint load while building the surrounding muscles — making it one of the more practical tools for knee rehabilitation. Results are best when a qualified instructor adjusts spring tension, range of motion, and alignment cues to match your condition.
What is the number one mistake that makes knee pain worse?
Allowing the knees to collapse inward (valgus) during any loaded movement—even with light resistance—is the most consistently harmful pattern. It overloads the patellofemoral joint and disrupts normal patellar tracking simultaneously, and it tends to go uncorrected when people train without supervision.
How many times a week should I do reformer Pilates for knee pain?
Two to three sessions per week is the generally supported starting point for musculoskeletal rehabilitation. That frequency builds strength and retrains movement patterns while leaving enough recovery time between sessions.
Can I do reformer Pilates after a knee replacement?
Yes, with physician clearance. The reformer's supported, low-impact format is well-suited to rebuilding range of motion and strength after surgery, with spring tension and load adjusted to your stage of recovery under close supervision.
What Pilates exercises should I avoid with knee pain?
Exercises that require deep unsupported knee flexion or single-leg loading should be deferred until the cause of pain is diagnosed and baseline strength is established. Your instructor will progress you based on what's pain-free — not a fixed exercise list.
How long does it take to see results from reformer Pilates for knee pain?
Many people notice meaningful pain reduction within 4–6 weeks of consistent sessions. Structural strength and lasting changes in movement patterns typically develop over 2–3 months. Timelines vary based on the severity and duration of the condition—post-surgical clients generally need longer.
If you're managing knee pain in Manhattan and want to explore whether reformer Pilates is right for your situation, The Pilates Room NYC offers private sessions tailored to injury recovery and rehabilitation. First-time clients can use code INTRO for 15% off their first one-on-one session. The studio is located at 150 West 28th Street, Suite 901, Chelsea. Reach them at 212-206-1827 or info@thepilatesroomnyc.com.