Introduction
According to the American Academy of Orthopaedic Surgeons, more than 450,000 total hip replacements are performed in the U.S. each year — and as that number climbs, more patients are turning to Pilates as part of their recovery. Pilates builds the deep muscular support that a new joint depends on, which makes it a sensible choice. The problem is that certain movements can work directly against healing when done too soon or without the right modifications.
Knowing which specific exercises cross into contraindicated territory during early recovery — and understanding the mechanics behind that risk — matters more than a class's "gentle" label. Some foundational Pilates movements are among the riskiest options post-surgery.
This guide covers the movement patterns to avoid, the safer alternatives that support recovery, and the timeline for returning to a full Pilates practice.
Key Takeaways
- Hip replacement removes the joint's natural ligamental stability, so surrounding muscles must compensate — precautions are non-negotiable
- Three core restrictions apply after posterior approach surgery: no hip flexion past 90°, no adduction across the midline, no internal rotation
- Avoid high-impact Reformer work, deep hip flexion exercises, rotation movements, and unmodified side-lying positions during early recovery
- Get surgeon clearance before starting or advancing any Pilates program post-surgery
- Private sessions with an instructor experienced in post-surgical rehabilitation are the appropriate starting format
Why Certain Pilates Movements Are Risky After Hip Replacement
The Anatomy Behind the Restrictions
The hip is a ball-and-socket joint — the femoral head sits inside the acetabulum and is held stable by ligaments, cartilage, and surrounding musculature. Total hip replacement removes the damaged natural joint and replaces it with a prosthetic. What it cannot immediately replace is the ligamental stability that held the original joint secure.
In the early weeks post-surgery, the prosthesis depends almost entirely on surrounding soft tissue and muscle to stay in position. Until those structures strengthen and the bone fully integrates with the implant, certain movement combinations create a direct path to dislocation.
The Three Standard Precautions (Posterior Approach)
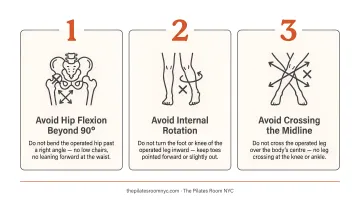
As defined by NIH StatPearls and clinical PT protocols, the three restrictions for posterior approach patients are:
- No hip flexion beyond 90° — bringing the thigh toward the chest past this angle risks pushing the prosthetic femoral head out of the socket posteriorly
- No adduction across the midline — crossing the operative leg past the body's center creates the same posterior dislocation risk
- No internal rotation — rotating the thigh inward is the third component of the posterior dislocation position, and particularly dangerous when combined with flexion
These three restrictions matter individually. When combined — flexion, adduction, and internal rotation occurring together — the dislocation risk increases substantially. Many Pilates exercises involve exactly this combination.
Anterior vs. Posterior Approach: Different Vulnerabilities
Not every hip replacement creates the same restrictions. The surgical approach determines which tissues were compromised:
- Posterior approach patients have the stricter early restrictions — flexion, adduction, and internal rotation are the primary concerns, typically for the first 6–12 weeks
- Anterior approach patients may instead need to avoid hip extension past 20° and external rotation past 50° in the early weeks — bridging and prone lying are often restricted as well
This difference matters enormously in Pilates. A movement that's safe for one patient may be contraindicated for another. Knowing your surgical approach isn't just useful information — it's essential.
Why the First 6–12 Weeks Are Critical
For patients with cementless implants (the most common type), the bone must grow into the implant surface for long-term stability. This process, called osseointegration, begins around 4 weeks post-surgery, with more mature bone integration continuing through 12 weeks.
During this window, high-torque movements and impact-loading forces can create micromotion at the bone-implant interface — the contact zone where new bone anchors to the implant — disrupting that integration process.
Altered proprioception after hip replacement also means the new joint provides reduced mechanical feedback. Follow precautions set by your surgeon and physical therapist. How a movement feels is not a reliable guide during this phase.
Pilates Exercises to Avoid After Hip Replacement
Risk in post-surgical Pilates is determined by movement pattern, not difficulty level. A beginner-labeled exercise that involves deep hip flexion or rotation is more contraindicated than an advanced exercise that keeps the hip in a safe, neutral position.
High-Impact Reformer Exercises
Avoid entirely in early recovery:
- Reformer Jumping / Jumpboard work — sudden loading and landing forces are incompatible with the healing bone-implant interface
- **Running on the Reformer** — the repetitive impact load stresses the new joint in a way that controlled strengthening work does not
- Jumping Jacks or plyometric variations — the combination of impact, abduction, and landing mechanics creates multiple simultaneous risks
The AAOS notes that high-impact activities can increase stress, wear, and loosening in hip implants. This applies both in early recovery and long-term.
Exercises Involving Deep Hip Flexion
The following movements bring the hip into flexion beyond 90°, directly violating the primary post-surgical precaution for posterior approach patients:
- The Frog — the combined hip flexion and external rotation routinely pushes the operative hip past the 90° threshold, even when the starting position looks controlled
- Unmodified Single Leg Circles and Double Leg Circles — the circular path can carry the operative leg into adduction and beyond 90° of flexion
- Rolling Like a Ball — requires sustained deep hip flexion and creates spinal loading that transmits force to the hip joint
These are foundational classical Pilates exercises. Because they appear in beginner programs, it's easy to assume they're safe. After hip replacement surgery, they are not.
Exercises Involving Hip Rotation
Rotational exercises stress the prosthesis in ways that can be invisible until dislocation occurs:
- Seated Twist — requires rotational force that transmits through the hip joint, particularly when combined with a forward lean that adds flexion
- Supine Leg Twist — internal rotation in supine directly triggers the posterior dislocation pattern
- Corkscrew — combines rotation, flexion, and spinal loading in a movement that hits multiple contraindicated patterns simultaneously
Posterior approach patients are especially vulnerable to rotation-based dislocation.
Even small rotational forces can displace the prosthesis before the surrounding soft tissue has stabilized.
Side-Lying Exercises
Two specific concerns apply to side-lying work:
- Side-lying Leg Circles — the rotational arc required can move the operative hip through internal rotation and adduction, regardless of where in the circle the movement occurs
- The Clam — while primarily an abductor exercise, the starting position and the hip rotation involved in opening the knee can stress healing tissue in the early weeks
Lying directly on the operative hip also compresses the surgical site and surrounding tissue at angles that may be unsafe until the soft tissue has healed. Timing and position selection matter here.
Any Exercise Requiring Unassisted Floor Transitions
Getting down to and up from a mat floor surface is one of the highest-risk activities in early recovery. The movement pattern requires hip flexion, single-leg loading, and balance — all while the joint's stability is still compromised.
Many mat exercises can be performed safely on a raised surface, such as a Cadillac or treatment table, which eliminates the floor transition risk entirely.
Across all of the categories above, the same rule applies: any exercise that produces pain around the new joint, clicking, grinding, a sensation of instability, or asymmetry should stop immediately.
Safe Pilates Movements to Try Instead
Early-stage Pilates that respects all three precautions can still be meaningful and effective. Options supported by AAOS post-surgical exercise guidance include:
- Ankle pumps and ankle rotations in supine — keeps circulation moving without any hip joint stress
- Heel slides — small-range knee bends in supine, stopping well before any hip flexion limit; keep the knee from rolling inward
- Theraband foot and ankle work — builds distal leg strength and neuromuscular connection with zero hip loading
- Modified Hundreds — feet flat on the floor or elevated on the Reformer footbar at a safe angle, arms pumping through a controlled range; keeps core activation without spinal flexion or hip compression
- Breathing with deep core activation — supine breathwork with gentle abdominal engagement actively supports recovery and places zero demand on the operative hip
Once the early circulatory and core work feels stable, hip abduction and hip extension exercises — performed with a short lever and within the surgeon's prescribed range — are the next priority. Both target glute strength without approaching rotation or flexion restrictions. Standing hip extension through a small range is especially useful: it loads the posterior chain in a functional position without stressing the joint.

At The Pilates Room NYC, instructors are experienced in adapting sessions to each client's specific recovery stage and post-surgical precautions — using the full classical apparatus, including the Cadillac as an elevated surface that eliminates unsafe floor transitions, so that every session stays within surgical guidelines while still building real strength and stability.
When Can You Start Pilates After Hip Replacement?
Most patients can begin a modified, supervised Pilates program somewhere between 6 and 12 weeks post-surgery, but two things need to be in place first: surgeon clearance, and an instructor who understands hip precautions and your specific surgical approach. Patients who practiced Pilates consistently before surgery tend to return sooner, since their baseline strength and body awareness reduce the learning curve.
The general recovery arc looks like this:
| Timeline | What's Appropriate |
|---|---|
| 0–6 weeks | AAOS-supported low-load movement only: ankle pumps, heel slides, supine abduction |
| 6–12 weeks | Modified supervised Pilates with surgeon clearance; strict precautions remain in effect |
| 3 months | Begin expanding movement while avoiding high-impact work and deep rotation |
| 6 months | More full participation with instructor-guided modifications |
| 12 months | Full Pilates participation typically possible |
The calendar is a guide, not a green light. A patient at the 6-month mark who still struggles with single-leg control or core stability isn't ready to advance — and pushing forward before those foundations are solid is how setbacks happen.
Common Mistakes When Returning to Pilates After Hip Replacement
Most errors happen not from carelessness but from reasonable-sounding assumptions. These three come up repeatedly.
Assuming "gentle" or "beginner" means safe. Rolling Like a Ball and Single Leg Circles are entry-level exercises — and both are contraindicated after posterior hip replacement. Perceived difficulty has nothing to do with movement safety post-surgery.
Advancing because you feel good. Hip replacement alters proprioception: the joint provides less mechanical feedback than a native hip. Pain-free sessions are not evidence that a movement is within safe parameters. The prosthesis can be stressed or loaded dangerously without any immediate sensation.
Attending group classes without full disclosure. A group instructor cannot monitor hip precautions or modify cues in real time for one participant — not without knowing their surgical history. Choosing a class led by someone without post-surgical experience compounds the problem. Private or duet sessions are the appropriate format until precautions are cleared and independent movement control is established.
Frequently Asked Questions
How long after hip replacement can I start Pilates?
Most patients can begin a modified, supervised program at 6–12 weeks with surgeon clearance. Patients who practiced Pilates pre-surgery and those who had an anterior approach may return sooner, while others may need more time based on healing and strength indicators.
What Pilates exercises should I avoid after hip replacement?
Avoid high-impact Reformer movements (jumping, running), deep hip flexion exercises (Frog, Rolling Like a Ball, Single Leg Circles), hip rotation exercises (Seated Twist, Corkscrew), and unmodified side-lying work (Clam, Side-lying Leg Circles) — particularly in the first 6–12 weeks post-surgery.
Can I do Pilates before my hip replacement surgery?
Pre-surgical Pilates builds the core stability, glute strength, and muscle memory that support faster post-operative recovery. Adapt exercises to your current range of motion and pain levels, and confirm they're appropriate with your surgeon.
Does the type of hip replacement surgery affect which exercises to avoid?
Yes. Posterior approach patients face stricter restrictions on flexion, adduction, and internal rotation; anterior approach patients typically have early limitations on extension and external rotation. Your instructor must know your surgical approach before designing any session.
Is it safe to use the Reformer after hip replacement?
The Reformer can be used safely with proper modifications — including keeping the footbar at a height that doesn't push the hip past 90° of flexion. High-impact Reformer work (jumping, running) and deep leg press work should be avoided until specifically cleared by your surgeon.
What signs should stop me from continuing a Pilates exercise after hip replacement?
Stop immediately if you experience pain in or around the new joint, clicking or grinding sensations, a feeling of instability or giving way, or any unusual asymmetry in balance or gait. Rest and consult your surgeon or physical therapist before resuming movement.