Most people reach for Kegels as the default fix. And while Kegels have real clinical support, only about 49% of women perform them correctly after brief verbal instruction — meaning half of people doing "pelvic floor exercises" aren't actually training what they think they are.
Pilates offers a different entry point. Rather than isolating one muscle group, it integrates the pelvic floor into a coordinated breathing, alignment, and core system. But the approach matters enormously — because a pelvic floor that's over-tight needs something very different from one that's weak.
This guide covers the anatomy, the evidence behind Pilates for pelvic floor health, specific exercises, key principles, and the mistakes most likely to stall your progress.
Key Takeaways
- Pilates trains the pelvic floor as part of the deep core system — not in isolation — producing more functional, durable strength
- A healthy pelvic floor needs both strength and the ability to fully release — over-tightness is as problematic as weakness
- Exhaling during exertion naturally lifts the pelvic floor — effective Pilates works with this breath rhythm throughout
- Pre/postnatal women, seniors, post-surgical clients, and those with stress incontinence benefit most
- Symptoms like leaking, pelvic heaviness, or pain during sex warrant evaluation by a pelvic floor physical therapist before starting Pilates
Understanding Your Pelvic Floor
What It Is and What It Does
The pelvic floor is a hammock-like group of muscles and connective tissue spanning the base of the pelvis. It supports the bladder, bowel, and uterus (or prostate in men), contributes to continence, and plays a direct role in spinal stability and sexual function.
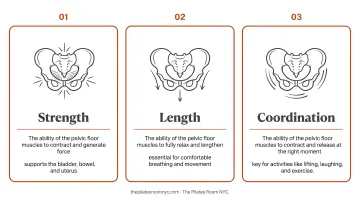
A healthy pelvic floor requires three things:
- Strength: contracting reliably under load — coughing, lifting, jumping
- Length: fully releasing and lengthening between contractions
- Coordination: responding reflexively to movement demands without conscious effort
Who's at Risk for Dysfunction
When any of those three functions breaks down, symptoms follow. Roughly 23.7% of U.S. women have at least one symptomatic pelvic floor disorder, with prevalence rising with age. Among postpartum women, the numbers climb sharply — one study of rural postpartum mothers found 56.9% reported moderate pelvic floor distress.
Common contributors include:
- Pregnancy and childbirth (instrumental delivery carries the highest odds ratio)
- Hormonal changes, particularly menopause
- Prolonged sitting — sitting 7+ hours daily is associated with urinary incontinence
- High-impact exercise without adequate core control
- Pelvic or abdominal surgery
Dysfunction doesn't always mean weakness. A hypertonic (over-tight) pelvic floor can cause pelvic pain, painful sex, constipation, and urinary urgency — and strengthening exercises alone will make it worse, not better.
Why Pilates Works for Pelvic Floor Strengthening Beyond Kegels
The Integrated Core Argument
Kegels train a single, isolated contraction. That has value — the Cochrane review confirms pelvic floor muscle training improves symptoms and quality of life for women with urinary incontinence. But the technique failure rate is high, and isolated training doesn't teach the pelvic floor to respond reflexively during real movement.
Pilates pairs pelvic floor activation with the transverse abdominis, multifidus, hip musculature, and diaphragm — training coordinated functional strength rather than a squeeze held in isolation.
Research comparing Pilates to standard pelvic floor muscle training has found comparable outcomes for postmenopausal women with stress urinary incontinence when voluntary pelvic floor contraction is included. Pilates isn't proven to outperform well-taught Kegels, but it provides a whole-body context that makes the training more functional and easier to sustain over time.
The Diaphragm-Pelvic Floor Connection
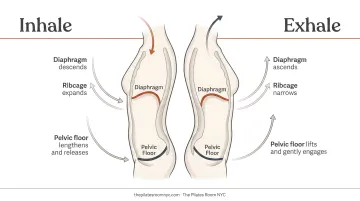
That whole-body context starts with breathing. The diaphragm and pelvic floor move together with every breath. On inhale, the diaphragm descends and the pelvic floor gently drops; on exhale, both recoil upward. This coordinated motion is well-documented in physiology research, and Pilates is designed specifically to harness it.
Every exercise cued with exhale-on-effort is using this reflex intentionally. It creates a natural pelvic floor lift without forced contraction — and it keeps intra-abdominal pressure (IAP) within a manageable range, rather than driving pressure downward as breath-holding does.
The Surrounding Architecture
Breath coordination is only part of the picture. Pilates also builds the surrounding structures that support pelvic floor function:
- Glutes and hip abductors — women with stress urinary incontinence show measurable weakness in hip external rotators compared to asymptomatic controls
- Hip adductors and deep spinal stabilizers — contribute to pelvic stability under load
- Postural alignment — reduces compensation patterns that contribute to dysfunction over time
At The Pilates Room NYC, this integrated approach shapes how Alison Johnson and the team work with prenatal, postnatal, and pelvic floor clients. Using the full classical apparatus — Reformer, Tower, Cadillac, Wunda Chair, and mat — every session treats core stability as one interconnected system.
Essential Pilates Exercises for Pelvic Floor Strength
Start with the foundational movements below. These exercises are sequenced by gravitational demand — floor-based first, loading increases as you progress. Advance only when you can maintain breath coordination and neutral pelvic alignment throughout without compensation.
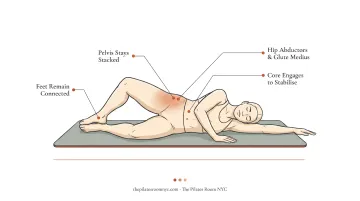
Shoulder Bridge (Pelvic Lift)
Setup: Lie on your back, knees bent, feet flat and hip-width apart, spine in neutral.
On an exhale, peel the pelvis and spine off the floor one vertebra at a time, squeezing the glutes at the top without overextending the lower back. Inhale to hold at the top, then exhale to roll back down with control.
The exhale-driven lift naturally recruits the pelvic floor without forcing a conscious contraction. The focus is on spinal articulation and glute engagement ; the pelvic floor responds as part of the system.
Clamshell
Setup: Lie on your side, knees stacked and bent to roughly 45 degrees, hips neutral and stacked.
Inhale to open the top knee; exhale to close it with control. The movement comes from the hip joint — the pelvis should not rotate.
This is not just a warm-up exercise. Research shows women with stress urinary incontinence have significant weakness in the hip abductors and external rotators this movement targets. Adding hip synergist strengthening to pelvic floor training produces better outcomes than pelvic floor work alone.
Dead Bug (Supine Leg Float / March)
Setup: Lie on your back, knees bent, feet flat.
On an exhale, brace gently through the low abdomen and pelvic floor and float one foot off the floor to tabletop. Inhale to lower it slowly. No bracing, no breath-holding — the effort should feel subtle. The lower back stays anchored throughout.
This trains the pelvic floor to respond to limb loading without IAP spikes. It's a foundational exercise for teaching the coordinated bracing response that Kegels alone don't develop.
Bird Dog
Setup: Start on all fours with shoulders over wrists, hips over knees, and spine neutral.
On an exhale, extend the opposite arm and leg simultaneously while keeping the pelvis completely level. Inhale to return. The quadruped position reduces gravitational load on the pelvic floor while still demanding coordinated deep core activation. This makes it well-suited for anyone earlier in recovery or with higher pelvic floor sensitivity.
From floor-based work, the deep squat introduces the first significant load — and one of the most effective positions for both activating and lengthening the pelvic floor.
Deep Squat
Setup: Stand with feet slightly wider than hip-width, toes turned out slightly.
Lower slowly into a deep squat (inhaling as you descend), keeping the chest lifted and spine neutral. Hold briefly at the bottom for 2–3 breaths, then rise on an exhale.
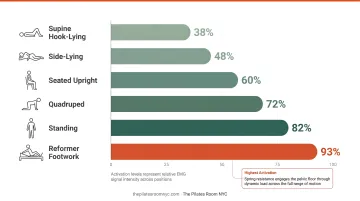
Research on female athletes found squat and quadruped positions produce some of the highest pelvic floor activation levels on record — parallel squat reached 151.40% MVC in one study. Beyond activation, the bottom position allows the pelvic floor to lengthen fully. For anyone whose pelvic floor is chronically tight from prolonged sitting, that lengthening component is as important as any contraction.
Key Principles That Affect Your Results
Breath Coordination
Exhale on the effort. Every time. This is the single habit that matters most in pelvic floor training — it creates a reflexive, natural lift at the moment of load without straining. Breath-holding (the Valsalva response) spikes IAP and pushes pressure downward. If you catch yourself holding your breath during an exercise, the load is too high or the movement is too complex.
Neutral Pelvic Alignment
Both a tucked pelvis (posterior tilt) and an exaggerated arch (anterior tilt) alter pelvic floor muscle tension and reduce training effectiveness. Research suggests posterior tilt may shorten fibers and reduce maximal contractility through length-tension effects. Maintain the natural lumbar curve with the pelvis level — this ensures the pelvic floor can work through its full range.
Release Is Not Optional
If your pelvic floor is hypertonic, more strengthening work will worsen your symptoms. Include movements that emphasize lengthening alongside contractive work. The deep squat and child's pose are the most accessible. The goal is equal capacity in both directions: full contraction and full release.
Managing Intra-Abdominal Pressure
Some classical Pilates exercises — double leg lowering, The Hundred with extended legs, full bilateral leg work — create significant IAP and are not appropriate starting points for someone with pelvic floor dysfunction. Begin with low-load, single-leg, or supported variations and progress gradually as control improves.
Two signals tell you IAP is exceeding what your pelvic floor can currently manage:
- Leaking during exercise — any involuntary loss, even minor
- Abdominal doming — a ridge or cone forming at the midline during movement
Either one means it's time to modify. Don't push through.
Common Mistakes to Avoid and When to Seek Expert Help
Gripping and Over-Contracting
"Engaging your pelvic floor" is frequently miscued — and the most common error is bearing down or over-bracing rather than performing a true upward lift. Given that nearly half of women perform Kegels incorrectly after verbal instruction alone, this problem extends even to people who think they've got the technique right. Feedback from a qualified instructor in the early stages is often what separates effective training from reinforcing the wrong pattern.
Skipping the Release Phase
Focusing only on strengthening while ignoring release work is how a normal pelvic floor becomes hypertonic. Pelvic pain, increased urgency, or worsened symptoms over time are common results. Build lengthening movements into every session — not as an afterthought, but as a core part of the work.
Progressing Too Quickly
Bilateral leg work, full planks, and jumping are high-intra-abdominal pressure (IAP) activities. Jumping to them before you've built foundational control is a common mistake that can worsen symptoms rather than resolve them. Leaking during exercise or abdominal doming are your body's way of telling you the progression is too fast.
When to Seek a Specialist
Anyone experiencing the following should consult a pelvic floor physical therapist before or alongside a Pilates practice:
- Pelvic organ prolapse symptoms (heaviness, dragging, visible bulge)
- Persistent stress or urge incontinence
- Pelvic pain or pain during sex
- Symptoms that worsen with exercise
At The Pilates Room NYC, Alison Johnson brings 26 years of experience working with prenatal and postnatal clients, including extensive work supporting pelvic floor strength and connection. The studio requires medical clearance before working with clients managing specific health conditions, treating Pilates as movement support that works alongside — not in place of — evaluation by a pelvic floor physical therapist.
Frequently Asked Questions
Is Pilates good for a weak pelvic floor?
Yes. Pilates integrates pelvic floor activation with breath, alignment, and full-body movement rather than training in isolation. Research comparing Pilates to standard pelvic floor muscle training has found comparable outcomes — making it a clinically supported option, particularly for those who struggle with isolated Kegel technique.
What is the difference between Kegels and Pilates for pelvic floor health?
Kegels are isolated contractions targeting only the pelvic floor. Pilates trains the pelvic floor as part of the entire deep core system — paired with diaphragmatic breathing, neutral alignment, and functional movement patterns — producing strength that transfers into daily activity more reliably.
How long does it take to see results from pelvic floor Pilates?
NICE guidelines recommend at least 3 months of supervised training for stress or mixed urinary incontinence, and at least 16 weeks for early-stage prolapse. Many people notice improvements in awareness sooner, but durable change requires consistent practice over time.
Can you do pelvic floor Pilates if you have pelvic organ prolapse?
Modified Pilates can be appropriate for prolapse but must be guided by a pelvic floor physical therapist and a knowledgeable instructor. The focus should be on gentle strengthening, symptom management, and avoiding high-intra-abdominal-pressure exercises.
Can men benefit from Pilates for pelvic floor strengthening?
Men have a pelvic floor and benefit from the same principles of breath, alignment, and load management. Clinical guidelines recommend pelvic floor muscle training for post-prostatectomy incontinence, and a 2023 meta-analysis confirmed its effectiveness for post-surgical urinary incontinence in men.
How often should you practice pelvic floor Pilates to see results?
Three to four sessions per week of 30–50 minutes is a reasonable target, with consistency mattering more than duration. Weaving pelvic floor awareness into daily habits — how you breathe during a lift, how you sit at your desk — accelerates progress beyond what formal sessions alone can achieve.